Path4HCPs
The hypothalamic MC4R pathway
The hypothalamus
The hypothalamus is an important region of the brain that controls diverse neuroendocrine functions, including regulation of energy balance, appetite, and body weight.1,2
It is a collection of interconnected nuclei located in the suprasellar region of the brain above the pituitary gland that controls:3,4
 Sleep, arousal, and circadian rhythms
Sleep, arousal, and circadian rhythms Fatigue
Fatigue Thermoregulation
Thermoregulation Thirst, salt, and water balance
Thirst, salt, and water balance Energy balance through the melanocortin-4 receptor pathway
Energy balance through the melanocortin-4 receptor pathway
What is the melanocortin-4
receptor pathway?
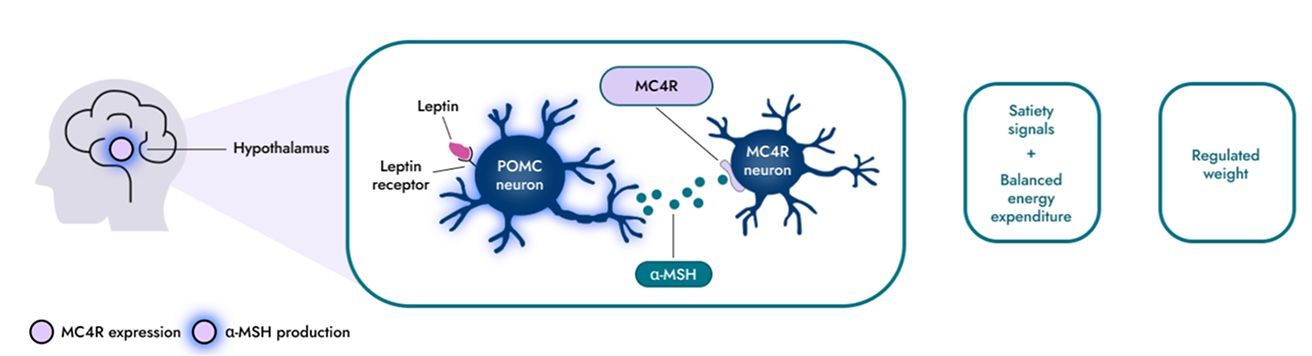
The melanocortin-4 receptor (MC4R) pathway in the hypothalamus is a key signalling pathway responsible for regulating hunger, food [caloric] intake, and energy expenditure, which consequently affects body weight.5–7
Proper regulation of appetite requires sufficient levels of α-melanocyte-stimulating hormone (α-MSH) that activate MC4R neurons, triggering a reduction in hunger and concomitant increase in energy expenditure.8,9,10
- 1
The MC4R pathway plays a key role in regulating satiety signalling, which involves neural activation within the hypothalamic region of the brain in response to leptin release from adipose tissue.
- 2
Proper regulation of satiety signalling requires sufficient levels of the neuropeptide alpha-melanocyte stimulating hormone (α-MSH), which binds to the MC4R.
- 3
MC4R activation by α-MSH controls satiety, food intake, and energy expenditure, all of which contribute to the regulation of body weight/composition.
Disruption of the
MC4R pathway
Rare hypothalamic MC4R pathway diseases can arise following physical injury or structural abnormality of the hypothalamus with MC4R pathway disruption and other functional impairment, or due to rare genetic variants directly disrupting the MC4R pathway.11
Disruption of the MC4R pathway may lead to decreased α-MSH production, impairing MC4R signalling and resulting in hyperphagia (pathological, insatiable hunger), decreased energy expenditure and significantly increased body weight, the key clinical features observed in patients with these diseases.11-13
Acquired hypothalamic obesity
Acquired hypothalamic obesity (aHO) is an accelerated and sustained weight gain resulting from physical injury or structural abnormality of the hypothalamus with MC4R pathway disruption and other hypothalamic functional impairment.14
This disruption of the MC4R pathway decreases the production of alpha melanocyte-stimulating hormone (α-MSH) and can potentially lead to aHO, which is associated with hyperphagia and decreased energy expenditure.11-14
Causes of aHO
Rare genetic variants directly disrupting the MC4R pathway: Syndromic and monogenic diseases
In syndromic and monogenic diseases, MC4R pathway signalling can be disrupted due to genetic variants upstream of the MC4R, leading to hyperphagia and early-onset obesity.7,12,30
Genetic causes
In complex syndromic diseases, such as Bardet-Biedl syndrome (BBS), MC4R pathway signalling is disrupted by genetic variants, where hyperphagia and early-onset obesity are often accompanied by neurodevelopmental delay or dysmorphic features, and organ-specific developmental abnormalities.12,30
Variants in at least 26 BBS genes and 4 modifier genes have been identified to disrupt LEPR signalling and subsequent activation of downstream MC4R-expressing neurons, potentially leading to hyperphagia and early-onset obesity.31
Learn more about:


Stay connected and get support when you need it
Access educational materials, updates, and expert insights or reach out if you have questions that haven’t been answered.
Stay informed
Sign up to stay up to date on the release of new resources
References:
- 1.
Farooqi IS. Biol Psychiatry. 2022;91(10):856–59
- 2.
Yeo GSH, et al. Mol Metab. 2021;48:101206
- 3.
Van Santen HM, et al. Eur J Endocrinol. 2023;188:10.1093/ejendo/lvad009
- 4.
Waterson MJ, and Horvath TL. Cell Metab. 2015;22:962–970
- 5.
Krashes MJ, et al. Nat Neurosci. 2016;19(2):206–19
- 6.
Cone RD. Endocr Rev. 2006;27(7):736–49
- 7.
Loos RJF and Yeo GSH. Nat Rev Gens. 2022;23(2):120–133
- 8.
Van Santen HM. Horm Res Paediatr. 2025:10.1159/000543544
- 9.
Dimitri P, et al. Front Endocinol. 2022; 13:8468803
- 10.
Garnett MR, et al. Orphanet J Rare Dis. 2007;2:10.1186/1750-1172-2-18
- 11.
Roth CL, et al. Obesity (Silver Spring). 2015;23(6):1226–1233
- 12.
Hochberg I, et al. Obes Rev. 2010;11:709–721
- 13.
Roth CL, et al. Diabetes Obes Metab. 2024;26:34–45
- 14.
Madsen PJ, et al. J Neurosurg Pediatr. 2019;24(3):236–245
- 15.
Van Santen HM and Muller HL. Endocr Rev. 2025:10.1210/endrev/bnaf025
- 16.
Ruiz S et al. Eur J Endocrinol. 2022;186(6):R79–R92
- 17.
Maas AI, et al. Lancet Neurol. 2008;7(8):728–741
- 18.
Crenn P, et al. Clin Nutr. 2014;33(2):348–353
- 19.
Mele C, et al. Int J Mol Sci. 2021;22:10.3390/ijms22052686
- 20.
Jais A and Bruning JC. J Clin Invest. 2017;127:24–32
- 21.
Goszyonyi G, et al. Brain Structure and Function. 2020;225:1459–1482
- 22.
Etemadifar M, et al. Care Rep Med. 2012:10.1155/2012/768580
- 23.
Cerbone M, et al. E Clinical Medicine. 2020;19:100224
- 24.
Hietamäki J, et al. E Clinical Medicine. 2022;51:101556
- 25.
Beales PL, et al. Obes Rev. 2025;26:10.1111/obr.13915
- 26.
Baldini G and Phelan KD. J Endocrinol. 2019;241:R1–R33
- 27.
Roth et al. Obesity. 2011;19:36-42
- 28. Fonseca ACP, et al. J Diabetes Complications. 2017;31:1549–1561.
- 29.
Huvenne H, et al. Obes Facts. 2016;9:158–173
- 30. Hampl SE, et al. Pediatrics. 2023;151(2).
- 31. Malhotra S, et al. J Pediatr Genet. 2021;10;194–203
- 32. Sivasubramanian R. and Malhotra S. Gastroenterol Clin N Am. 2023;52:323–332.
- 33. Argente J, et al. Lancet Diabetes Endocrinol. 2024;13(1):29–37.
- 34. Poitou C, et al. Eur J Endocrinol. 2020;183;R149–R166